Every radiologist knows the friction. You open a case, expect the priors to hang alongside the current study, and instead you see nothing — or a partial, irrelevant list. You go hunting. Minutes disappear. Often, the cause is not missing data. It is non-matching data. The priors are there, but the system cannot match them to the current study because the names do not line up.
Behind that small daily irritation sits one of radiology informatics’ oldest unresolved problems: study description naming. This is where study description normalization becomes critical. It does not make keynote slides, but it quietly determines whether priors load correctly, whether hanging protocols trigger, whether AI tools process the right images, and whether dose registries and outcome studies can aggregate data across sites. This article explains what study description normalization actually is, why it matters, and what modern radiology platforms do about it.
One exam, a thousand names
Consider a single common study: CT of the abdomen and pelvis with intravenous contrast. In any given European hospital network, the same exam might appear in the RIS or DICOM header as “CT ABD/PEL WO” (meaning without IV contrast at one site, without oral contrast at another), “CT ABDOMEN PELVIS C+”, “CTABD-PELVIS CONT”, or as free text dictated by a clinician. The work by Mabotuwana and colleagues in mapping institution-specific descriptions to RadLex Playbook entries documented exactly this problem — similar exams performed at different institutions carry different codes and descriptions, created at institutional level rather than regionally or nationally.
This matters because every downstream system — PACS, viewer, AI triage, priors retrieval, registries — depends on being able to recognise that all those strings refer to the same exam. Without normalisation, each system makes its own best guess, and inconsistencies propagate.
Why it breaks priors
Priors retrieval typically looks for matching study descriptions and modality combinations across the patient’s imaging history. When naming is inconsistent, the matching fails in predictable ways:
The radiologist fixes this manually — typing patient names into search, scrolling through lists. Each instance costs a minute or two. Across a department, it is hours of misplaced time per day.
- A prior from 2022 labelled “CT ABDOMEN & PELVIS” does not match a current study labelled “CT ABD/PEL WITH CONTRAST”, even though both are the same exam for clinical purposes.
- An outside prior imported from a different hospital’s PACS carries that hospital’s chargemaster codes, which your local viewer does not know how to interpret.
- A scanner configured with a vendor-default description overrides a department protocol, producing two different strings for the same exam performed on the same day.
What RadLex and LOINC actually do
The Radiological Society of North America (RSNA) developed the RadLex Playbook as a standardised vocabulary for radiology procedure names. Each procedure has a unique identifier (RPID) and a set of attributes — modality, body part, contrast, technique — expressed consistently. In 2017, RSNA and the Regenstrief Institute completed a harmonisation project, producing the unified LOINC/RSNA Radiology Playbook, described in detail by Vreeman and colleagues in the Journal of the American Medical Informatics Association in 2018.
The result is a universal terminology that maps a local procedure description — “CT ABD/PEL WO” — to a standardised code. Once a hospital’s procedures are mapped, priors retrieval, registries, AI routing, and cross-institutional analytics all use the same canonical reference.
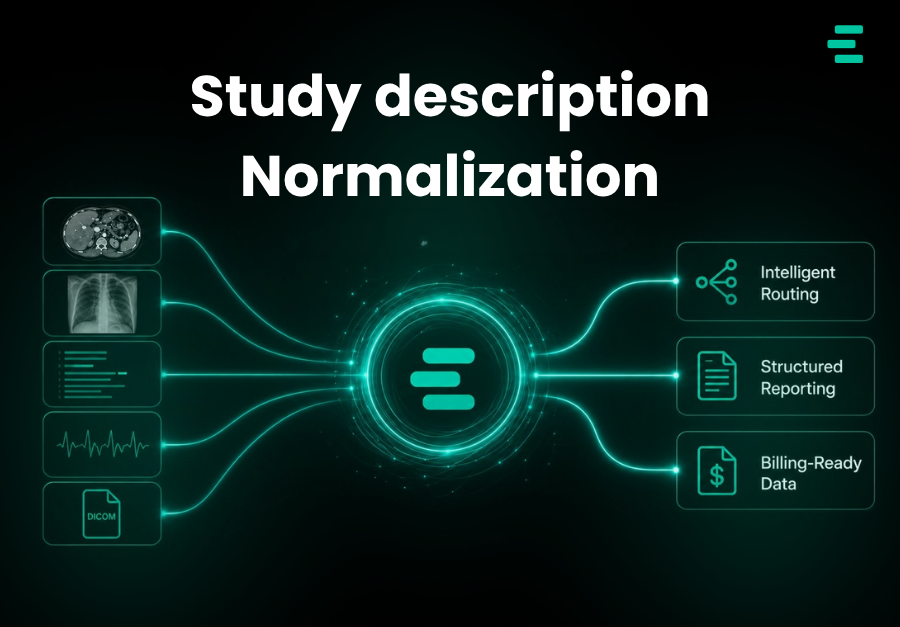
What Study normalisation desription unlocks
The payoff of study description normalisation is not one feature — it is a cascade of improvements across the workflow:
- Reliable priors retrieval — the radiologist opens a current study and the correct priors hang automatically, without manual hunting.
- Dependable hanging protocols — protocols trigger consistently because the viewer can trust the classification of the exam it is rendering.
- Registry participation — for example, the ACR Dose Index Registry depends on standardised procedure naming to produce comparable benchmarking.
- Better AI training data — machine learning models need consistent labels; normalisation is foundational for building useful internal datasets.
- Smoother teleradiology — remote readers work across sites, and normalised descriptions reduce the cognitive overhead of constantly adapting to local naming conventions.
Where normalisation sits in a modern workflow
Done well, normalisation happens in two places: at ingest and at viewing.
At ingest
The best time to normalise a study description is when the study enters the system. Tagging engines that classify and standardise metadata at ingest — using rules, vocabulary mappings, and AI image analysis when text metadata is ambiguous — catch errors before they propagate downstream. Evorad’s evoTag is one example of this pattern: automated classification that normalises study labels at entry, giving downstream orchestration and routing tools clean data to work with.
At viewing
At the point of reading, priors matching should tolerate imperfect upstream data. A diagnostic viewer that uses both structured metadata and semantic matching — for example, Evorad’s evoViewer, which pairs with automated patient history analysis to surface clinically relevant priors and prior measurements — closes the gap when historical studies carry inconsistent labels. The belt-and-braces approach (normalise at ingest, tolerate mess at viewing) is what actually produces a reliable prior-retrieval experience in real hospitals with real messy data.
The bottom line
Study description normalisation is one of those plumbing problems that shows up as a daily irritation and a long-term productivity tax. Hospitals that treat it as a serious informatics project — mapping to RadLex/LOINC, tagging at ingest, using viewers that tolerate upstream inconsistency — get back minutes per case and hours per week of radiologist time. For imaging leaders under workforce pressure, that is not a small win. It is one of the most leveraged investments available.
References
- Mabotuwana T, Lee MC, Cohen-Solal EV, et al. Mapping Institution-Specific Study Descriptions to RadLex Playbook Entries. Journal of Digital Imaging. 2014;27(3):321–330. doi:10.1007/s10278-013-9663-y
- Vreeman DJ, Abhyankar S, Wang KC, et al. The LOINC RSNA radiology playbook — a unified terminology for radiology procedures. Journal of the American Medical Informatics Association. 2018;25(7):885–893. doi:10.1093/jamia/ocy053
- Radiological Society of North America. RadLex Radiology Lexicon and Playbook. Available at: https://www.rsna.org/practice-tools/data-tools-and-standards/radlex-radiology-lexicon