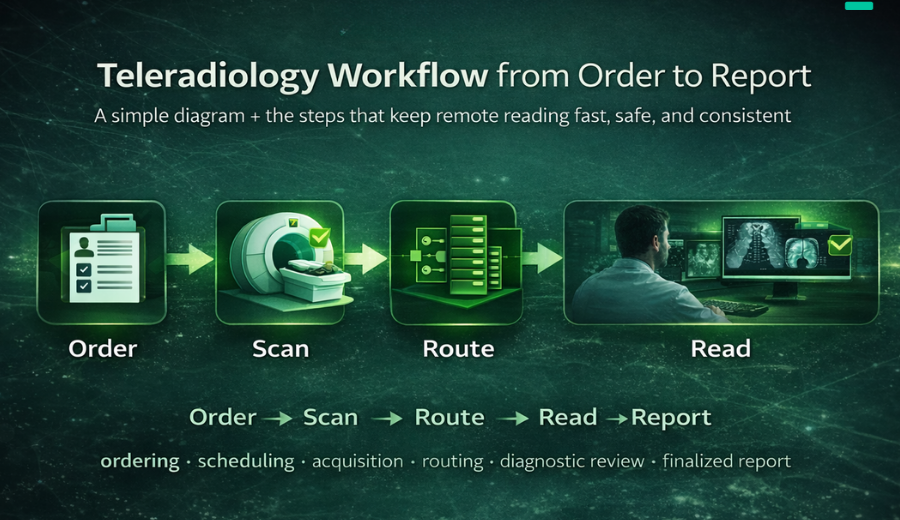
Hanging Protocols (and Why They Matter to Radiologists)
Ask a radiologist what makes a diagnostic viewer “good,” and somewhere in the top three answers you will find: hanging protocols that work. It is not a glamorous piece of clinical software. It is one of those quiet layers that is invisible when it works and infuriating when it does not.
But hanging protocols matter more than most hospital leaders realise. Across a department reading 400 studies a day, the cumulative minutes of manual image re-arranging — dragging, resizing, flipping, reloading priors — translate into hours of radiologist time per week. In an environment where the European workforce shortage makes every radiologist-hour precious, that is not a minor optimisation.
What a hanging protocol actually is
A hanging protocol is a set of rules that tells the viewer how to display a study when it opens. The term comes from the film era, when technologists physically hung films on a lightbox in a particular order so the radiologist could read them without rearranging. The Society for Imaging Informatics in Medicine (SIIM) defines a hanging protocol as the arrangement of images for optimal softcopy viewing — essentially, the radiologist’s preferred layout encoded in software.
The DICOM standard formalises this through the Hanging Protocol Service Class and Hanging Protocol Composite Information Object Definition (IOD), specified in DICOM PS3.17. In principle, this allows hanging protocols to move between viewers from different vendors. In practice, most vendors implement extensions and proprietary features, which is one reason radiologists lose hanging protocols when hospitals switch PACS.
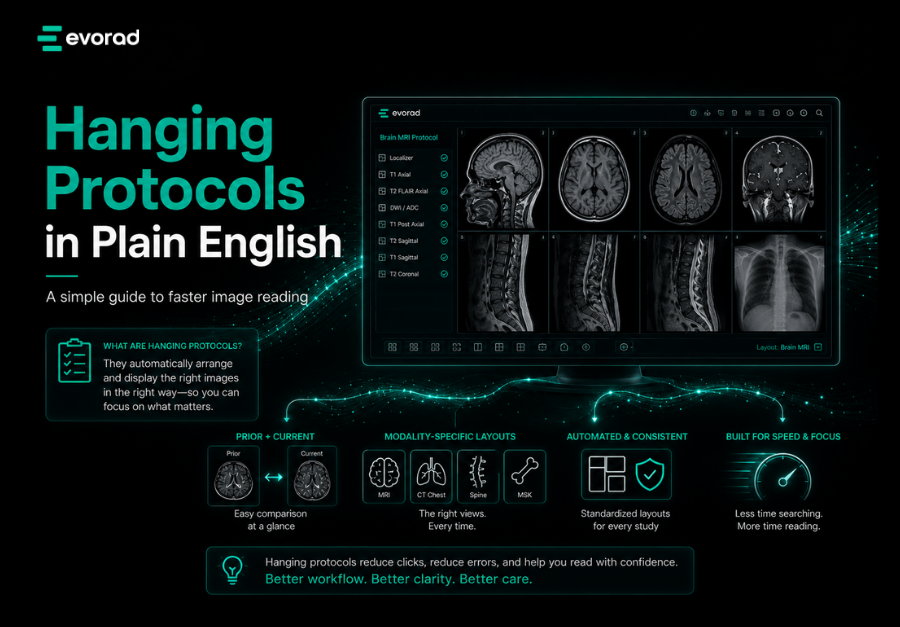
What a good hanging protocol does on every study
For the radiologist, a working hanging protocol does five things automatically — all before the first click:
When that works, the radiologist opens the study and is ready to read. When it fails, they spend 30 to 90 seconds rearranging before each case. Multiply that across a working year and the productivity delta is enormous.
- Lays out the current study series in the radiologist’s preferred screen arrangement (e.g., axial, coronal, sagittal in a predictable grid).
- Retrieves and displays relevant priors side-by-side for comparison.
- Applies modality-specific settings — window/level presets, orientation, grayscale inversion, measurements.
- Handles laterality and body-part conventions consistently (e.g., mammography right-to-left versus left-to-right).
- Manages multi-series studies intelligently — grouping related sequences, separating contrast phases, flagging incomplete series.
Why hanging protocols break
Despite the DICOM standard, hanging protocols fail frequently. There are three common reasons:
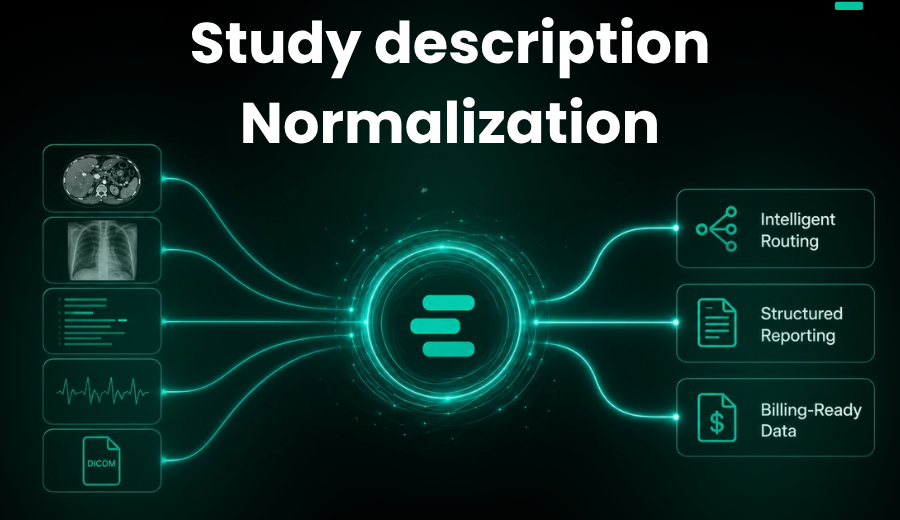
Inconsistent DICOM metadata
Hanging protocols depend on clean metadata — modality, body part, series description, view position, laterality. When the technologist fills in a free-text series description differently on Tuesday than on Monday, the protocol does not trigger. Multiply this across a 10-hospital network with different scanner vendors and the failure rate compounds.
Multi-vendor studies
Priors from outside the institution — sent via media, CD import, or image exchange network — frequently carry non-standard metadata. The current study may hang perfectly while the prior from an outside hospital loads in default layout, forcing manual rearrangement every time a comparison is needed.
Viewer limitations
Some viewers allow only modality-level hanging protocols. Others support series-level, but not exam-level or user-specific customisation. The more limited the protocol engine, the more fallbacks the radiologist needs to perform manually.
What a modern viewer should deliver
For a diagnostic viewer to handle hanging protocols well in 2026, it needs to do more than follow DICOM PS3.17 to the letter. It needs:
- Exam-level adaptation — protocols that respond not just to modality and body part but to procedure indication and clinical context.
- Per-user customisation — individual radiologists read differently; their protocols should follow them across workstations.
- Intelligent prior matching — so a current chest CT opens alongside the most relevant prior chest CT, not a random abdominal study from three years ago.
- Graceful fallback — when metadata is missing or non-standard, the viewer should use image analysis to infer enough to place the study sensibly, rather than dumping it in default layout.
- Clean integration with study description normalisation — because reliable hanging protocols are only as good as the data feeding them.
A practical example
Evorad’s evoViewer is one example of a viewer built with smart hanging protocols that adapt to modality, series, and exam-level workflows, combined with precision tools for annotations, measurements, and 3D visualisation. The broader point for radiology leaders evaluating viewers: don’t let hanging protocol support be glossed over in procurement. Ask to see it in action with your own real studies — including your messiest outside priors.
The quiet economics of getting this right
It is worth putting a number on this. A radiologist reading 40 studies a day loses about 20 minutes per session to manual re-arrangement when hanging protocols fail consistently — roughly 30 seconds per study on the cases where the viewer dumps the study in default layout. Across a team of 20 radiologists working five days a week, that is over 30 radiologist-hours lost per week. Whether a department values that time at locum rates, contracted consultant rates, or simply in throughput terms, the annual figure is material.
The reverse is also true. A viewer where hanging protocols reliably work — including on imperfect metadata and outside priors — is one of the clearest “quiet wins” available in radiology IT. It does not show up in a brochure headline, and it will not generate enthusiastic testimonials. But it will generate radiologists who stay, turnaround times that hold, and a department that feels different to work in.
The bottom line
Hanging protocols are one of those unglamorous details that separate a viewer radiologists tolerate from one they actually like. In a market where workforce shortage has made every minute of a radiologist’s time valuable, tolerating a viewer that breaks hanging protocols twice a day is a silent productivity tax. For hospital and imaging centre leaders, putting hanging protocol behaviour on the PACS/viewer evaluation checklist—with real-world test cases—is a small discipline with outsized returns.
References
- Society for Imaging Informatics in Medicine (SIIM). Hanging Protocol. SIIM Open Terminology Project (otpedia). Available at: https://siim.org/otpedia/hanging-protocol/
- National Electrical Manufacturers Association. DICOM PS3.17 2024: Explanatory Information — Hanging Protocols. Available at: https://www.dicomstandard.org/current
- Radiological Society of North America. RadLex Playbook Series. Available at: https://www.rsna.org/practice-tools/data-tools-and-standards/radlex-playbook-series